
Multiomics Trends in 2026
From Siloed Data to Systems-Level Insight
Spatial biology reveals tissue architecture that single-cell sequencing alone cannot be resolve. Pharma is using integrated omics to ask questions that single-modality data cannot be answered. And AI has moved from an optional analytical layer to infrastructure. Three trends define this inflection point, and each carries specific evidence worth examining.
Key Market Signals
The commercial and scientific momentum behind multiomics is increasingly visible in both market growth and large-scale translational datasets. The figures below highlight several signals shaping the field in 2026.

In 2026, multiomics is not waiting for a breakthrough. The capabilities exist, and what is changing is that they are converging. Spatial transcriptomics, single-cell profiling, AI-driven integration, and large clinical datasets are no longer advancing independently — they are reinforcing each other, producing a qualitative shift in what the field can ask.
For most of its history, the central constraint was data generation: not enough resolution, not enough throughput, not enough scale. That problem has not disappeared, but it is no longer the binding one. The rate-limiting step today is interpretation — turning complex, heterogeneous datasets into something a researcher or clinician can act on. Three developments define how that plays out in 2026: spatial biology revealing tissue-level structure that single-cell sequencing alone cannot capture, AI becoming the infrastructure on which multiomics integration depends, and pharma moving from exploratory interest into active deployment.
Trend 01: Spatial biology is making tissue architecture legible
Here is the thing about single-cell sequencing: it tells you what a cell is doing, but not where it is doing it. And in biology, location is not a footnote — it is often the whole story. The tumor microenvironment is a geographically organized ecosystem. Which immune cells get suppressed, which fibroblasts activate, which cancer populations survive — these outcomes are shaped by proximity. Bulk and single-cell assays average all of that out. Spatial technologies put it back.
A July 2025 study published in PNAS, edited by Rakesh Jain at Harvard Medical School, applied spatial multiomics to hepatocellular carcinoma tissue and identified an "interface zone" between tumor cells, cancer-associated fibroblasts, and immune cells that had never been described before — showing that fibroblasts in that zone drive immune suppression by secreting lactic acid. That mechanism, and its implications as a therapeutic target, was simply not visible without simultaneous spatial transcriptomic and metabolomic data. No prior approach could have found it.
The field is not standing still within oncology. A Frontiers in Immunology review (October 2025) documented how spatial and single-cell integration is enabling systematic reclassification of tumor–immune microenvironment architecture and beginning to predict which patients will respond to checkpoint blockade.
The field is also moving fast beyond oncology. A March 2025 study in Nature Medicine by van Olst, Simonton, and colleagues at Northwestern University and the Singapore Immunology Network used spatial transcriptomics and single-cell RNA sequencing to map the neuroimmune response inside Alzheimer's amyloid plaques, identifying how the TREM2–APOE axis responds in microglia and characterizing lecanemab's effects directly in brain tissue.
 Spatial multiomics is not a refinement of single-cell sequencing. It is a different kind of question — one about how the geography of tissue governs the biology of disease.
Spatial multiomics is not a refinement of single-cell sequencing. It is a different kind of question — one about how the geography of tissue governs the biology of disease.
Trend 02: AI has become the infrastructure, not just a tool
For years, AI in multiomics meant running a model on top of a finished dataset. The more significant shift is the emergence of biological foundation models — large architectures pretrained on tens of millions of cells that can be fine-tuned for specific tasks with far less data than conventional methods require. A research group working on a rare disease cohort of a few hundred patients could not previously train a reliable multiomics integration model. A pretrained model changes that arithmetic entirely.
scGPT (Cui et al., Nature Methods, Feb 2024), pretrained on 33 million cells, is currently the only foundation model integrating scATAC-seq alongside transcriptomics — genuinely multi-omic, not just multi-dataset. Nicheformer (Tejada-Lapuerta, Schaar et al., Nature Methods, Oct 2025), trained on 110 million cells across 73 tissues, established empirically that models trained only on dissociated data cannot recover spatial microenvironment complexity. And Geneformer, extended into a therapeutic target discovery framework (Nature Protocols, April 2026), uses attention weights to surface disease-specific candidate targets — closing the loop from model to actionable biology.
The AI question in multiomics is no longer whether machine learning helps. It is which architectures to build on — and whether they can explain themselves well enough to be trusted in a clinical context.
That last point matters more than it typically gets credit for. Regulators, as documented in npj Digital Medicine (March 2026), are now evaluating AI-enabled omics tools on interpretability and biological plausibility — not just accuracy. A model that cannot expose its reasoning is scientifically limited and regulatorily stuck, no matter how well it performs on benchmarks.
Trend 03: Pharma and diagnostics have moved from interest to deployment
The clearest sign that multiomics has crossed from research into industry is not market size — it is which questions it is now being asked to answer. In May 2025, Illumina and Ovation.io released the largest commercially available clinical multiomics dataset built around GLP-1 receptor agonist patients: 25,000 whole genomes, 9,500 proteins profiled per sample. It was designed specifically around the non-response problem — roughly 40% of Type 2 diabetes patients do not respond adequately to GLP-1 therapies — and made available to the pharma community to find out why. That is multiomics as a commercial decision-support tool, not a research project.
The M&A picture confirms the direction. Illumina's $350M acquisition of SomaLogic (January 2026) combined sequencing with aptamer-based proteomics at commercial scale. Its Mayo Clinic partnership is a product development agreement for rare disease diagnostics — not a research collaboration.In diagnostics, Natera's Signatera holds broad Medicare coverage and is under PMA review as a companion diagnostic, with a March 2026 review in Frontiers in Molecular Biosciences documenting how ctDNA detected colorectal cancer recurrence 4–10 months ahead of clinical imaging in prospective studies. The next generation combines ctDNA with methylation, RNA, and protein signals — a multiomics assay with tissue-of-origin specificity no single analyte can match.
When a 25,000-patient dataset combining whole genomes and 9,500 proteins is built specifically to understand drug non-response, that is not exploratory science. That is multiomics as commercial infrastructure.
Outside oncology, a 2025 analysis in Mayo Clinic Proceedings: Digital Health showed that combining genomic, epigenomic, and proteomic markers improved antidepressant response prediction in psychiatry — a domain that has resisted precision medicine for years because single-gene approaches explain too little variance. Prospective validation at scale remains ahead, but the direction is clear.
What the field has not yet solved
None of the above means multiomics is a solved problem. The bottleneck has shifted from data generation to interpretation — but building that interpretive infrastructure comes with its own structural constraints.
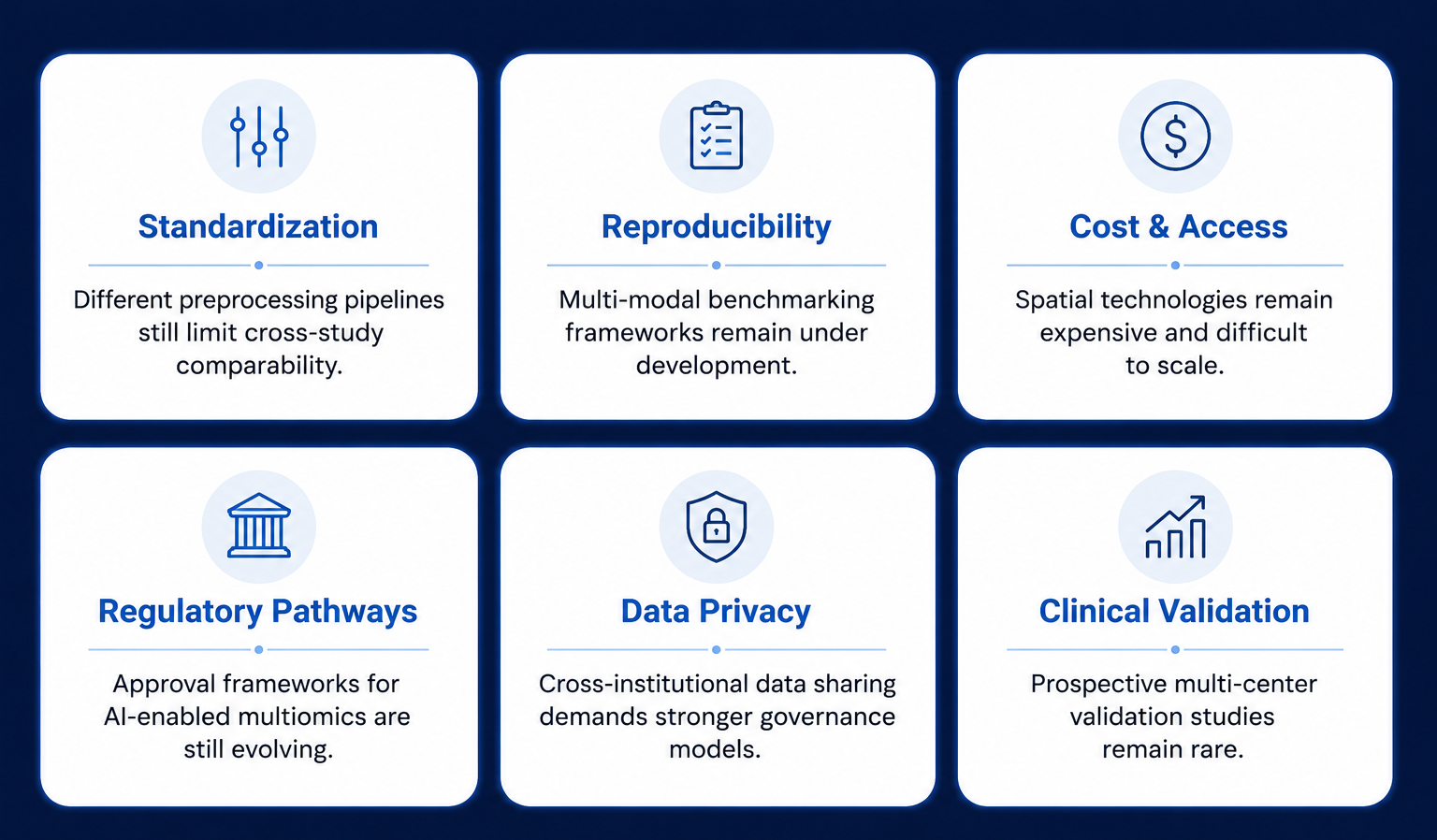
These challenges do not diminish the promise of multiomics; they define the work that remains. The future of the field will depend as much on validation, standards, and analytical infrastructure as it does on new technologies.
Conclusion
Five years ago, multiomics was defined by the challenge of generating data — throughput, storage, modality-specific pipelines. Those problems are tractable now. The harder problems are the ones that replaced them: building models that generalize across heterogeneous biological contexts, making spatial data actionable in a clinical workflow, validating a multiomics biomarker through regulatory processes that were not designed for it.
The HCC interface zone study, the Alzheimer's spatial proteogenomics work, the GLP-1 dataset, the Signatera MRD trajectory — they all point to the same thing. Value in multiomics no longer lies in generating more data. It lies in building the infrastructure — spatial platforms, foundation models, validation frameworks — that turn data into decisions. That is a harder and more consequential problem. It is also where the leverage sits.
Biology has always been a data problem. What changes in 2026 is that the data problem is becoming an interpretation problem — and interpretation, unlike sequencing, does not get cheaper simply by building faster instruments.
👉 aimed analytics is building analytical infrastructure for the multiomics era, helping researchers transform complex biological datasets into interpretable, reproducible, and actionable insights.